Last updated: April 9, 2026

 December 7, 2024
December 7, 2024Timestamps:
00:00:33 – Tiers of Longevity Intervention
00:29:14 – Calorie Restriction – Beneficial for Humans?
00:39:00 – Biomarker Tuning vs. Habit Changes – Which is Better?
00:13:11 – Unaging Challenge 2025 Update
Michael Lustgarten: Hey everyone, today’s guest is Crissman, channel regular, Crissman Loomis. And if you don’t know who Crissman is, he’s the face and brains behind unaging.com. So check it out. So with that in mind, welcome Criss and what’s on the agenda for today.
Crissman: Thanks Mike, it’s always a pleasure to talk to you. So we’ve got a few things. I’ve had some revelations or new thoughts over the past couple of months and I’m looking forward to sharing them with you.
So let’s go over our topics. So the things I think we can talk about today. First of all, is I’ve done some analysis, and crunched some of the numbers to go into the tiers of longevity.
So we can see what are the top interventions or habits that you can do that’ll give you the most life. Then after we talk about that a bit, I thought we could talk about calorie restriction in humans. For a long time, it’s been thought that this is one of the primary ways that you could extend life in humans.
And I want to talk about some of the recent findings on that. After that, we can go talk about biomarker tuning versus habit changes. So which of them is better? What’s the better focus to take your look at?
And then finally, I’d like to give an update on the unaging challenge for 2025 and how things are going with the early adopters. So that’s the layout. Sound good for you?
Michael: Yeah, longevity tiers. looks like two and three. looks like two and three is challenging the conquer aging or die trying approach. So yeah, let’s get into it, right? Should be good.

Crissman: Okay, so starting with the tiers of longevity intervention. So the research here is basically pulled from various sources. So I’ve gone over, as I’ve been writing my unaging blog over the years, the various different ways that you can change your all-cause mortality. So I find that I don’t like to get caught into the weeds of changing the chance of cancer or cardiovascular. I want to look at the big picture.
And say, overall, what are the best interventions that you can do to live the longest amount of time? And I’ve gone over health habits, I’ve gone over diet habits, I’ve gone over habit habits like sauna and other things, and as much as possible, quantified them.
So I took those numbers that I had figured out and then ran them through an actuarial table. This is based off of assuming someone who is a 40-year-old male.
If you’re older than 40, you won’t quite get as much benefit. If you’re younger, you’ll get more. If you’re a woman, you’ll get little bit less because you’re already going to live a little bit longer than men.
But this then gives an idea of how much benefit you could get for any particular intervention. So you’ll notice also that there’s a green side of it and then also there’s a gray side of it.
So the green side is basically what the average American or developed country person would get from doing this intervention. So for some of these, for example, like eating vegetables or things, a good number of people fortunately already do eat some vegetables.
So the net benefit of it is not that great. But of course, if you look at this and you’re not doing it at all, say for instance, if you are not doing any walking,
Then increasing your walking will have more of a benefit. You can capture not only the green benefit of it, which is over seven years, but also you could get additional benefit as well. And for some of the interventions, the point actually is that you want to do less of them.
Down number three on the list is smoking, which we know has negative impacts in multiple areas. So quitting smoking will then get you, by stopping it will give you the benefit of extra years of life.
Crissman: So going ahead and jumping into then the two top tiers, the S tier and the A tier interventions.

In the S tier, we have the number one intervention, which is walking. Basically, just simply walking about 12,000 steps a day, 10,000 is good. And the first, of course, 8,000 steps are the most impactful. You can gain about another seven years of life.
It’s amazing that a lot of the gurus that we hear about talk about how important it is to do the other activities because they’re seems more challenging and not everyone does them, but many people think of it as the first thing for longevity.
But the number one intervention that gives them over about a 75 % reduction on cause mortality is walking about 12,000 steps every day. So I give that its own tier is the S tier. And after that, then we start to go into the A tier.
And you’ll notice that the A tier is thBegin activating plugine other physical interventions for the most part. It’s things like high intensity interval training called HIIT here on the chart. Doing aerobic exercise, which is where you’re going at more of a steady state, but at a high enough rate that it’s difficult to breathe.
Your heavy breathing. And then also strength training once a week to build up the muscles as well. There are a few other habits here. As I talked about smoking, unfortunately I…
I don’t feel like I need to tell too many people that smoking isn’t healthy for you, but smoking isn’t healthy for you. And another one there is sauna, which is somewhat less known, unless you’re living in Finland, that it also is one of the top actually of the A-tier interventions that will give you quite a bit more life.
It’s about a 35 % reduction or more just going to the sauna for about 10 to 20 minutes several times a week. So this then covers the S tier and the A tier. And then after that, then we come to the B tier.

And it’s interesting because the B tier is kind of a bunch of the very top food habits that maybe you don’t actually think of. Very at the top of the list there, I call it DRIP, which is my abbreviation for drip coffee.
It’s important that it be drip coffee as opposed to an espresso because some of the oils in an espresso or a latte are not as healthy. And another equivalent of that basically is tea.
Crissman: If you do both of these things, you don’t get twice the benefit. They seem to overlap in some ways, especially in the caffeine, which is about half the benefit of either tea or coffee.
And other interventions we have here is whole grains, which is one of the most reliable interventions because you can have up to three to four servings of whole grains and that could be whole wheat pasta, cereal, granola, whole wheat bread, or other things.
It just seems to continue to be healthy throughout. There is not as much of one dose is good and the second dose is not as good. It seems to be a consistent benefit the more of it you eat. In contrast to that, the next intervention is nuts.
But nuts are a one-serving intervention. Basically, all you can eat is one serving of nuts, 30 grams, actually not even a full ounce, about 20 grams of it, and you get the full benefit. As far as gram-for-gram life, there’s nothing that beats nuts. And olive oil is another popular alternative to this that basically gives the same benefit. Underneath that, we have the only supplement to grace the list, which is glucosamine.

The chondroitin oftentimes comes together, but it seems like the glucosamine is the actual one with the benefit. There are questions about how effective it actually is for the primary purpose, which is joints and knee treatment.
But it’s very inexpensive, it’s heavily tested with very few side effects, although glaucoma is one of the possible side effects. So if that’s a concern for you, I don’t recommend it. And it’s shown to have a significant decrease in premature death.
And then the last one that’s sort of on the borderline between the B and the C tier is fish. Having about one or two servings of fish, up to 200 grams, also gives a significant increase in lifespan.
So then we get to the C tier and this is kind of interesting.

I think this is like the sin tier if you will. The things here are oftentimes talked about as maybe not healthy and there are already a lot of people who don’t take that much of them. Here we have things like processed meat, sugary beverages, and any beverage that is only bringing sugar like a soda or iced tea can be overly sweetened.
Crissman: Orange juice is another one that seems healthy, but really is just liquid sugar for the most part. These things, unfortunately, will shorten your life, and so cutting them out can give you additional lifespan.
Legumes or beans also appears on this list as one of the good things that can be done with one or two servings, around 40 to 80 grams a day. Eggs is okay at the rate of about half an egg a day or an egg every other day or so, but over that…I don’t really know whether it’s the cholesterol or whether it’s what it is, but it’s shown in the observational studies that basically having an egg or more a day starts to reduce your expected lifespan.
And the same is true of red meat, you can see for red meat that while not many people eat that much of it, there are some people who eat a lot of it. That’s why the bar extends quite a bit over to the left side for people who need to eat more meat than is healthy for them.
The last one in this tier is flossing. Fortunately, most people do floss, but if you don’t floss, can be a significant increase in your overall longevity. Then we get to the D tier.

Sometimes I think of this as a distraction tier. The things here, while they do extend your life, they’re often times oversold and many people are doing most of them, the beneficial amount already. We have both fruits and vegetables appear on this list.
But most people are already eating a serving or two of fruits a day and the observational studies don’t show that much benefit beyond one or two servings a day.
Decaffeinated coffee is not as healthy as caffeinated coffee, but if the caffeine is doing a thing for you, this is better than nothing for people who are sensitive to caffeine. Another one here, the peppers, this is red peppers. So if you eat a whole red pepper about once a month, once every other week or so, it shows significant benefits as far as longevity.

Some of the other vitamins or spices as well, such as garlic or some of the others, or turmeric can have a similar benefit. And then also we have things in here like brushing your teeth. Again, most people do this. So the additional benefit for most people is telling people what they already know, that brushing your teeth every night gives a longevity benefit.
Crissman: Brushing your teeth in the morning is good for breath and other things, but it doesn’t seem to be tied to reducing all-cause mortality. And then again, instant coffee, which also has benefits.
Even if it’s caffeinated, you can get the caffeine benefit out of it, although the polyphenol and other benefits seem to disappear, so it’s not as significant. And then there are some things that don’t really make a difference.
Refined grains, white bread, and other things, it’s not negative. If eat it, doesn’t shorten your lifespan, but doesn’t give you additional time either. And the same is true of poultry, which is sort of a neutral protein source.
So those are the tiers of longevity. Do you have any questions or comments about that, Mike?
Michael: Yeah, so I got a whole bunch of questions and comments. So first, hopefully, you can provide all the references, you know, so that we can then we can put it in the video’s description or the pinned comments, and then people can check out the studies just so they know that you’re not just pulling these data at thin air, right?
Crissman: Yeah, mean, the foods are pretty much all in one study. But I’ve written, I think around coming up on 100, I think more than 50 blog articles. for instance, if there’s an oral microbiome, we’ll then tell you about the flossing, the dental care, and other things. But I’m happy to provide those links, and then people can take a look at it.
Michael: Yeah, cool. right, and then, so just starting from the top, right? So you’ve got walking basically is the top, top of the top, even beating the potential gain in lifespan for aerobic training, strength training, even HIIT, right?
So how does that mesh with the VO2 max studies where, okay, I get 12,000 steps, you’re gonna have a reduction or 12,000 steps are significantly associated with reduced all-cause mortality risk as is higher aerobic capacity, muscle strength, and obviously, HIIT is a component of that. But how do you square the circle with basically higher VO2 maxes, which can’t be achieved by walking?
You can walk all you want, and you’ll have a higher VO2 max relative to someone who’s sedentary. But people who are engaged in regular vigorous exercise training will have higher VO2 maxes. And a higher VO2 max will be associated with a lower all-cause mortality risk relative to someone who’s walking, right? So how do you square that circle for walking’s potential lifespan gain here on your chart versus the VO2 max studies?
Crissman: So each of these components, as I’ve gone through my studies, are independent of each other. the fact that you can gain this much additional expected life or have this much of a reduction in premature death from walking is in no way reducing or competing with the benefits that you get from having a higher VO2 max.
Just as eating lots of whole grains is going to increase your lifespan without affecting your VO2 max at all. It’s the same thing for walking, going for a long walk seems to have outsized benefits, even among people who do aerobic exercise as well.
And this was one of the interesting things for me is that it really is a different thing. So in the unaging challenge, one of the challenges that early adopters are finding is that getting 12,000 steps a day takes a long time.
And they’ve already been going through the challenge and they’ve already been doing things like doing aerobics and high-intensity interval training, but you can’t count those steps towards the walking because they’re separate and distinct. So I consider to be in overall fitness and longevity, walking is a different bucket if you will, than the other exercises.
So, I don’t think they conflict and they’re additional in the benefits you can get from them.
Michael: All right. So the way you’ve got it then is to make sure you’re doing some amount of aerobic and strength training, some hit, but then also get 12,000 steps in per day. That’s how you’re interpreting that. All right. I prefer.
So this gets ahead of the bait slash fight slash, know, whatever you want to call it, but you know, I prefer greater, I prefer greater specificity, right? If you were a VO2 Max, just use that as an example, or your muscle strength, arms, and legs pick.
Crissman: Yes.
Michael: Pick a grip strength, squat, deadlift, whatever it may be. If you’re at the top 1 % or elite of the elites or the best that your body can handle, would you even need walking, right? So then it gets the idea of specificity, right?
Can you use a more quantified approach or conversely, if you’re doing, I don’t know, 20,000 steps, do you need any aerobic training or strength or HIIT, right?
So, you know, I get the general recommendations, but then how do you…personalize that so that you’ve got a more specific recommendation for not just walking verse or how much walking within the context of the other health-promoting behavior.
Crissman: Yeah, you’re hitting on something that’s foreshadowing our upcoming discussions as well, because there isn’t a biometric that changes by walking.
Right? If I do my aerobics or something, then I can tell my VO2 max has increased, and my resting heart rate has gone down. If I do strength training, I can lift more, literally, and have grip strength and other things. But you’re absolutely right for walking.
There really isn’t a metric aside from how many steps you walk that tells you that you’ve done it and yet the results in all-cause mortality are unmistakable.
It’s one of the things that I struggle with just for the reason that you’re saying is, well, what did it do for you? And yet in study after study, this is very reliable with a very low P factor repeatedly replicated that the people who walk the most live the longest.
Michael: In those studies though, it seems like it’s one or the other though. I don’t know that there’s a quote-unquote healthy control group where, you know, they’re running on the treadmill at, don’t know, whatever speed and, know, doing heavy compound lifts and then also walking 12,000 steps.
It seems like that’s one or the other where you’ve got a general population that happens to walk a lot, a little or less, and isn’t doing any of the vigorous training. So I think it’d be interesting to look at head-to-head studies, you know, for walkers versus the high-performance athletes.
And then how much walking do you need if you’re a high-performance athlete? Is it none? What amount is it? And then conversely, would some amount of regular training above walking be beneficial for those who walk a lot, right? So that’s how I would interpret it.

Crissman: Yeah, think, I think there, I don’t have the study off the top of my head, but I think there was a study that actually looked at specifically the aerobic fitness and the walking fitness and found that they were additive on each other.
Of course, for all these things, as a spoiler, if you did everything perfectly on all of these tiers, the last additions are not going to get you any life anyway. So as you talk about someone who’s already an elite athlete, if you already have an elite athlete, let’s say who’s eating an outstanding meal and also goes to the sauna, has never smoked, et cetera, you’re probably right.
That person probably has maxed out already what they could get. Virtually no one lives past 110. You get your own Wiki, you get an entry on the Wikipedia page if you live past 110. So it definitely is true that you can max it out with some of the other things if walking takes up too much time or it’s not something that you enjoy. There’s definitely the ability to pick here, but if you have to pick one or two, one of them should be walking.
Michael: Yeah, which then also gets a dose, right? What do you think about the overtrained phenotype? Because if you’re doing five, six days of an hour, an hour a day of strength and cardio and everything else, and then are adding 12,000 steps, which is another six miles of volume, you’re basically now training three hours a day instead of one hard training per day.
Are you overtrained? And is that overtrained? Will that overtraining phenotype lead to less strength and cardio performance in your training move, you know, your training activities, right?
Crissman: Mm-hmm.
Michael: And then will that negatively impact health and lifespan? So what do you think about that?
Crissman: Well, there’s an acclimatization time to getting used to walking. I have a walking desk as I’ve appeared in one of our first videos walking on my treadmill underneath my desk that I work on. And a regular day for me is going to be 30,000 steps.
That’s kind of standard. Honestly, I don’t think I’m getting benefited after the first 12 or 15,000 as we talked about, but I’m still a little on my desk and I don’t have a chair. So away I go.
But I think that the walking, the benefit of it is, is that you don’t, it doesn’t wear you out. Like if I walk for two hours and then do my exercise or I just do my exercise, I don’t notice any difference in my overtraining or readiness to do the exercise.
I find that in a couple of things, there seems to be a trade-off between them. For example, in aerobic exercise, if you’re just doing aerobics, the max period is somewhere at about five hours or so, and after five hours of solid aerobics like if you’re running more than five hours a week you’ll begin to edge into the overtrained and the longevity benefits begin to disappear.
The total high-intensity time once that gets to around an hour and a half you’re already to getting the overtrained point and again you’ll start to see the longevity benefits start to go away
And also you’ll start to see VO2 max go down as you’re literally over-trained. And that’s also, I’ve seen that it come up in a few studies, but for walking, I’m not aware of any particular number where they said, Whoa, Whoa, don’t walk that much.
When they go out to the tribes and things, right? And the primitive people who are living the hunter-gatherer life, walk all day long and they’re fine.
Michael: But then it’s that that still goes back to they’re doing one or the other. The walkers aren’t doing vigorous training and probably vigorous training or doing some walking, but not a lot of walking.
Everybody suggested circling back to the acclimatization and acclimation to the higher training load, you know, adding walking to an already pre-existing training approach. so I don’t think everybody can adapt to a higher training volume. And I think there are limits to that.
So just use an analogy from sports. So in baseball, you’ll have pitchers who will start their careers thinking they’re going to be starting pitchers. And a starting pitcher generally, well, in the past, in the 70s and 80s, used to throw 250 innings. So when they’re 18 years old, they would start throwing a lot of innings.
Well, some of those pitchers couldn’t throw a lot of innings. So now, instead, their arms and their physiology just can’t handle it. So instead of throwing 250 innings, and for some teams, it takes many years to figure out that they’re not a 250 inning workhorse they’re only capable of throwing 60 to 70 innings before they start breaking down.
So I think the same idea translates to, you know, human physiology when it comes to exercise and longevity. mean, more is not necessarily better. And then it becomes, you know, what kind of horse are you? It seems like you’ve got, you know, keep training, your body’s gonna keep adapting no matter what.
Unfortunately, I have the mindset to do that, but my physiology does not react, you know, well in that case. So yeah, just that nuance of trying to, then that gets the dose. How do you figure out if you’re in the overtrained zone, regardless of what is quote unquote associated with it in published studies, right?
Which goes back to heart rate variability, resting heart rate, and trying to get closer to the dose. That’s the only weak spot that I see in the broad-based epi studies is there’s just no specificity on dose. Like for example, how many whole grains, right? Is it?
Crissman: Mm-hmm.
Michael: Is five servings? Is it three servings? Maybe my physiology is one serving, right? Or conversely, the nuts. Maybe it’s not one serving. Maybe my physiology is better when I have three or four, but you’d have to actually measure biomarkers and do that, you know, iterative correlation process over time to see how much is truly optimal at the individual level.
Maybe some people thrive not eating any of these foods and just on, you know, 400 grams of animal products have fantastic biomarker data and everything else and feel better and, know, so.
I appreciate the epi studies. think that’s a good guide, you know, there’s got to be a more titrated way to get a dose.
Crissman: Yeah, we need more loose cartons out there to be measuring every gram and everything and doing different things, right? Obviously these are done in observational studies and individual variation kind of gets blurred into the average. So yeah, for some of those people, maybe it was five servings of nuts and for some of them, it was even half a serving.
Michael: Yeah. And then in most of the large epi studies too, even though you’ve got very large populations, I think it’s biased towards the unhealthy user and not necessarily the healthy user. The healthy user is so small, so small of a group that I wonder if it just gets buried in a noise. And then you’re looking at basically quote-unquote sick versus sicker people.
Right. So, I wait a couple of, a couple of other interventions that I don’t see on your list would be leanness, not necessarily BMI, but you know, so for example, you know, you could eat all of the quotes unquote real food. I mean, basically this approach distills down to the Jack Alain approach, eat real food and exercise, right?
But, you know, you could eat all of these foods, but if your BMI is 35, you know, versus something less, and that’s not to poop on people who are 35, they’re just more likely to be metabolically unhealthy, just as an example. You know, so I think leanness, but then even that’s a debatable topic, right? Is it?
Based on BMI, probably not. And then it’s like, what body fat percentage do you want? Which then divides it even further, which should be on the list potentially. Visceral fat, visceral fat, you know, increases during aging, is associated with insulin resistance and a whole bunch of bad health-related outcomes.
So that could be on the list. I’ve got a couple more too. Sleep quality, sleep duration, and quality. So sleep duration goes down with age. Slow-wave sleep goes down with age, which is associated with dementia risk. And then last but not least, sunlight, right?
How much sunlight to get not just vitamin D, but the red and near-infrared light, which can potentially improve mitochondrial function to some degree and glucose levels based on at least one RCT? So that would add those variables. I got a couple of other variables too, but what do you think?

Crissman: I think you’re absolutely right about those. In some ways, I’ve tried to focus on the things that I thought were most actionable. Body fat for whatever it’s worth, although thanks to modern drugs and GLP-1 and other things, it’s more actionable than it was before.
But going to someone who’s overweight and saying, hey, why don’t you not be overweight, it’s not an easy ask. It’s a lot of work, to be honest.
So I did do some research on that one. know that staying within a lean weight is about, probably about a, it’s about a B tier, I think. And if you’re overweight, then losing just a couple of pounds even, you don’t have to get down to like a low body weight. The metabolic change correction is much faster than the weight loss.
So the encouraging thing is if you are overweight, just starting on the road to losing weight, gives you the health benefits almost immediately. It takes a lot longer to have the scale reaffirm what you’ve done, but the benefits come more quickly and that’s about a 10 % recovery in reduction in premature death.
The sleep one, for example, that’s about a 10 % or so increase in all-cause mortality, and mostly the big problem there is people sleeping too long. If you’re sleeping, say, five hours instead of seven hours, it’s about 3%. It would definitely be D-tier.

think sleep is overrated as an intervention. The visceral fat stuff, I don’t have numbers on that one. I haven’t done that one again. That one’s really hard to say. You should fix your visceral fat, right? mean, losing a particular kind of fat is even more difficult, I think, than losing overall fat.
So there are definitely some things that could be added here. I watched your recent podcast and I’m excited to get into that I’ll be following up with that myself as well to see how I think the numbers shake out.
Michael: Air quality, air quality, so air pollution, that’s another one which is associated with mortality risk and then also water purity, right? So if you’re drinking lead-contaminated water and don’t know it, that’s potentially bad, at least for biological age.
But then even there, there’s nuance, how clean and pure should the water be? Are you stripping everything, reverse osmosis, and then you gotta add back in the vitamins and minerals to make it more palatable and less soft, right? So I would add those to air air air pollution and water probably.
Crissman: One of the ones that I would like to add to the list that I struggle with myself is the social contact measures. We know that loneliness kills and that’s one that it’s really hard to quantify and get good data on.
Are you happy? How lonely are you? Stress is another one that I would add if I could get better numbers on it to quantify how much stress people are under and then see how that affects their overall longevity. These are things that we know have a big impact.
Maybe they would bump walking off of the S tier, but it’s very hard to get good numbers on them and to quantify them effectively.
Michael: Cool. All right, ready for topic number two?
Crissman: All right, sure. See calorie restriction, is it beneficial for humans? Right, so before we get into this, I want to emphasize that we’ve been doing these podcasts now a few times. And I think that there are a lot of things that we agree on, as we’ve already seen just when we were talking about the tiers.
For instance, I think we both agree that diet is important. I think we both agree that exercise is good and that supplements have lower value. Wouldn’t say any value, but it’s not the first thing to look at when trying to live a longer life. Does that seem fair? Okay. Right, so…
Michael: Yes. But, I mean, it depends though, because some people could say that supplements with a hundred, taking a hundred or 150 supplements is doing something, but the foundation diet exercise, but then I would also add sleep, air quality, water pollution, some amount of sunlight exposure. mean, sure. Yes. Yeah.
Crissman: We got more podcasts to go. You know, I mean, those are the things we agree on and we’ve talked about them a few times, but I think it’s time we got down to brass tacks and had a fight about some of the things that I don’t think we do agree on. So, are you ready to go at it?
Michael: Born Ready.
Crissman: All right, one minute.
Crissman: Let’s do this. Ha!
Crissman: I need to arm her up. I don’t want to hurt you too much. I think we still have some future podcasts ahead of us. But see, you’ve been talking about this calorie restriction and you’ve been eating fewer calories than you need to. But the thing is, is that you also gave, and hosted a presentation from Kamil Poblis, if I remember his name right.

So he visited your podcast and he talked about the impact of short-lived controls on calorie restriction. Basically as he went through it, he found that the calorie restriction that they show in the animals only works in the small animals, like basically the lowest-weight animals.

So for any one of the four interventions they do, whether it’s in yeast cells fruit flies, or mice, the top 10 % have no benefit from calorie restriction at all. And these are even in the animals. And it’s only in the bottom 10 % by weight that get any benefit from it. And so a natural question out of that is, are humans more like fat rats or like lean rats?
How long do we live for our size? Well, this has already been answered.
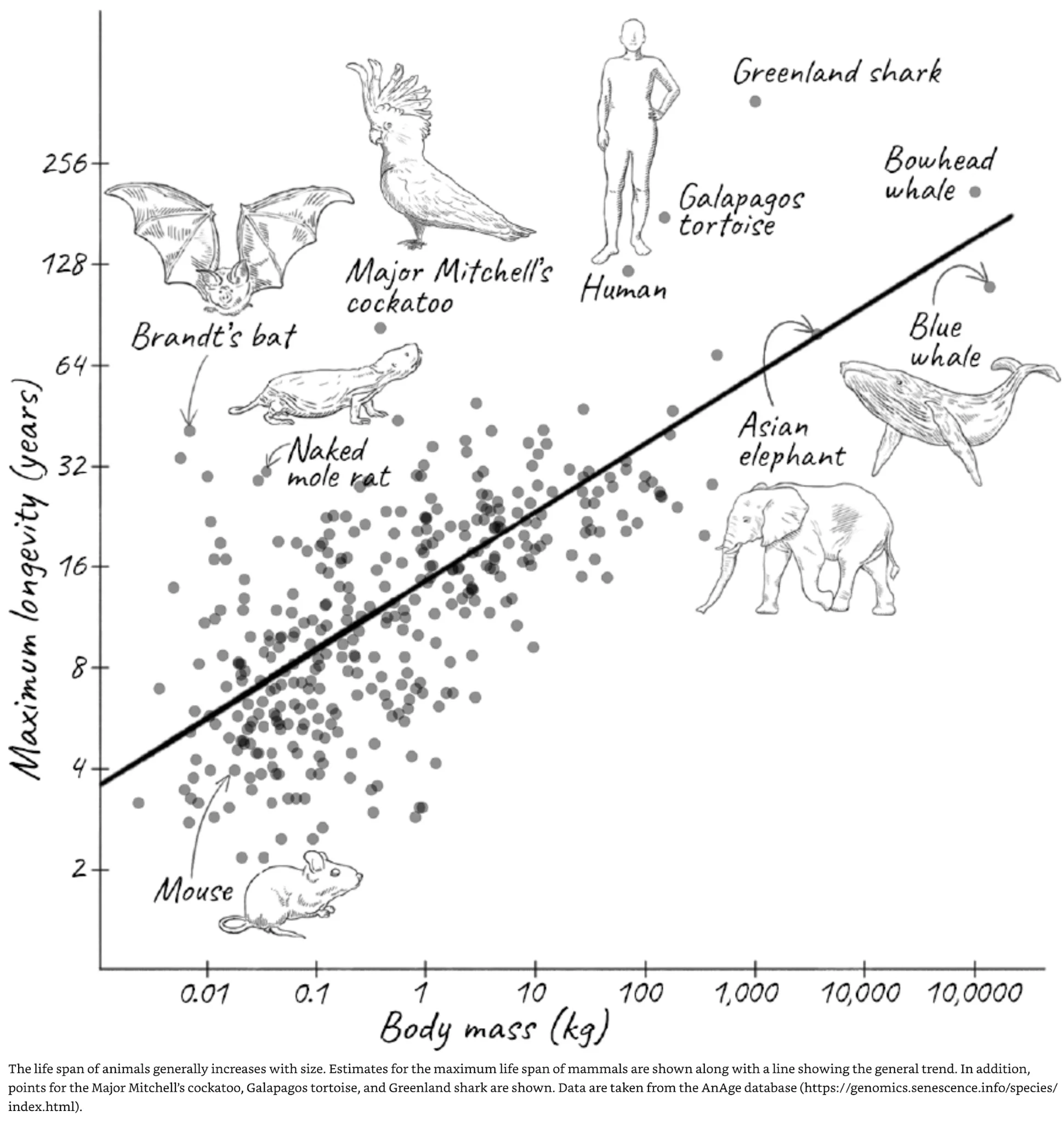
Here’s a statistical analysis that went through and it measured every animal they could find on how long it lived versus how much it weighed. And you can see down there in the lower left, we have mice underperforming the amount of time that you expect them to live given their body weight.
And then all the way at the upper top of it, we see humans who live much longer than you would expect for our physical size.
In fact, we live five times as long as would be expected just based on our weight. So when we’re looking, trying to compare ourselves to these fruit flies or other things, none of them live anywhere as long as a human does just based on how long you would expect something to live based on their weight.
Crissman: Then if we go further into that, one of the natural places to look is you’re thinking about longevity. You mentioned this is one of the things that should be on the tiers is the mortality based on body weight for a human. If it was true that eating low calories for an extended period of time was the key to longevity, then naturally you would be seeing that the people who weigh the least would then live the longest. But we don’t see that at all.

In fact, the people who weigh the least actually die 50%, and have a 50 % higher all-cause mortality than people who have a normal BMI of between 20 and 25.
So it only starts to go up as we mentioned before, when you started to get into a heavy BMI. But if you’re in a normal range, there’s really not that much benefit from eating fewer calories. And you could say, well, I’m doing calorie restriction, I’m not just losing weight.
Well, of the people who are doing calorie restriction, almost all of them have very low BMI, an average of around 18 or so, which is at the point that it’s significantly increased alcoholism mortality. this has already been done, and data has already been cleaned to remove the smoking people. One way to lose weight, unfortunately, is to smoke.
It’s also been corrected for the level of activity and exercise and class and age and other things. So this is basically saying that the humans that are living in the normal range can’t get any additional benefit just from trying to reduce their calories and live a life of deprivation. You wanna go ahead and give a swing back?
Michael: Yeah. So if we’re starting with the 900-day rule, the major takeaway from that paper too, was that CR was one of the few interventions to consistently allow mice to live longer than 900 days.
So if 900 days, if median lifespan of 900 days is a short-lived control, CR was one of the few interventions where consistently the mice lived longer than 900 days. And if I can, if I can share the screen here.
So I can show that data. Can’t share. You’ve got to give me shared privileges.
There we go. All right, hang on real quick.
Yeah. So if you look at one of the recent studies that just came out I don’t know. Wait, let’s see if you can see what I see. Let me go full.
So this study just came out and there for those who haven’t seen it videos on the channel, the importance of this study and not to say this is any different from the 900-day rule, but it it’s additive because this is recently published. So it wasn’t available when Camille’s group published his data.
Michael: Anyway, this study included 960 mice. that’s a key point because when you look at any lifespan studies, if you’re two groups or however many groups have eight mice per intervention or controls, it’s not adequately powered to look at lifespan.
So each of these five groups eats as much as you want to add lib. One day of fasting, two days of fasting, 20 % CR, 40 % CR, five groups. 960 mice in total, divide that by five. That’s how many mice were in each group, a lot of mice.
Grant, and also it’s in female mice, so I can’t say anything about male mice in this study. So when you look at the 900-day rule, that’s about 30 months right here, median lifespan. So compared to the ad-lib, you can see that relatively short-lived was, but an increase in lifespan relative to the short-lived ad-lib, eat as much as you wanted, both one and two days of fasting.
So maybe you can cross off one and two days of fasting as being potentially relevant because it increased lifespan relative to the short-lived controls who live shorter than 900 days. You could also make that same claim about, or actually where now where you start to see the lifespan curve go beyond 30 months, or sorry, sorry, now, then even 20 % CR, you can see 20 % CR median lifespan is right at 30 months, 900 days.
So there too, you could say, okay, 20 % CR, no extension of lifespan. If you use the 900 day rule, and basically, your ad-lib, those are short-lived controls. But then you can see 40 % CR very clearly way past the 30-day rule.
So you could say, OK, the 40 % CR is pretty extreme. Almost nobody can handle that. And where I prefer nuance to everything you just mentioned is that while it’s true that absolute CR is probably bad, you can’t say E, as little as possible, have a BMI of 18, right? That’s something I’ve never proposed ever and I never would propose, right?
It’s finding the body weight and body composition that’s associated with your best biomarker profile in terms of how that biomarker looks, how those biomarkers look in terms of youth, and their association with all-cause mortality risk. So in other words, it used to be calorie restriction with optimal nutrition, C-R-O-N.
Crissman: Yeah.
Michael: I’d add to that C-R-O-N and optimal biomarkers. So Cronob, right? So I guess I just turned the new phrase. And it’s probably a terrible name.
We can come up with other names. to highlight that point, just using this study again as an example, when using the, not the 30-day rule, but taking it even a step further and looking at mice that lived in any group past 35 months, which clearly beats the 30-day rule.
So you can see that even in the mice that ate as much as they wanted, there was still a pretty good amount that lived longer than 35 months and got close to more than 40 months, which is long-lived for a mouse.
Obviously, as you go up the groups, there are more mice in both CR groups that lived past 35 months. But the authors of this study then ask, which biomarkers are associated with a longer lifespan without even looking at if the animals were CR or not?
Right, so the one day of fasting, they weren’t CR. Two days of fasting ended up being CR. So you have two groups that are essentially not CR and three groups that ended up being CR. So in terms of biomarkers that were associated with a longer lifespan, regardless of which group those mice were in, having higher levels of lymphocytes at a relatively young age, 16 months, was associated with a longer lifespan.
And on the other side, having a higher RDW, which as many people know on the channel is a major predictor of biological age using Dr. Morgan-LeBain’s biological age test. Phenal age, having a higher value for that, regardless of group designation, was associated with a shorter lifespan. So these data aren’t just in mice.
This story is similar in people. The RDW increases during aging, this is in people again, and a relatively higher RDW is associated with an increased all-cause mortality risk.
And conversely, lymphocytes decline during aging, just like they did in that giant mouse study with lower levels of lymphocytes being associated with an increased all-cause mortality risk. just to go back to your original point, it isn’t an absolute CR where lower is better, get your BMI as low as possible.
I look at it as, finding the magnitude of CR that’s best associated with your most youthful and quote-unquote healthy lowest all-cause mortality risk biomarker profile.
Michael: But then also, how do you feel? Because if you’re tired and hungry, you’re probably too extreme, right? So, and it may be different for everyone, you know, just as another example on this, just to add more context.
So there’s a genetic model of obese mice called the OB-OB mouse, where they’re fat little mice. So if you calorie restrict them, and I’m not talking about like 40 % CR, just a mild calorie restriction, their lifespan is as long as, you know, 40 % CR, so you could say how is that possible? And they’re still fat.
They have a genetic model of obesity, which ties back into your point that there’s something about eating below your set point. And what that is may be different for everyone. Is it 10%, is it 30 %? For me, around 22, 23 % CR may be best. If I go below that, my biomarkers like lymphocytes, for example, start to look aged. but, allergy restricting the OB-OB mouse leads to a lifespan as long as classical CR, but yet they’re not at a body composition or body weight as the classical CR group.
So there’s something about the, the, a mild, even a mild energy restriction, that can, maybe it’s turning on quote-unquote pro longevity pathways. But then to add one last point, whether or not that will translate in people who know we’ll see, right? But, there’s no way to know. We’ve got to do the 70-year longitudinal study.
Crissman: Yeah, well, we’ve got to… Well, first of all, as I mentioned before, I’m not at all confident that mice results then can be extrapolated to people. That’s one of the big questions that’s not clear. And I think that the answer to that, especially because the strains of mice that we have been interbred for years, they’re domesticated, if you will, and they’re used to getting tons and tons of food.
When they try these…calorie restriction experiments with wild strains that are just recently brought into the lab. They find no benefit of the calorie restriction among mice or other things or with animals that are not tamed, like, basically our yeast cells or fruit flies or the things that have spent generations in captivity. the study is interesting though. and that one actually came out after 900, the 900-day study. Interesting. All right.
I’ll have to take a look at it.
Michael: Yeah, so wait, so to add to us more context. So I’m not saying that let’s use the animal studies and just marry that as an idea and hold onto it with faith and, and absolutism. And I’m going to have a BMI of 18 and I’m going to live super long because of it and do nothing else. Like I think that approach is flawed, which goes back to the biomarkers, right? If you’re on some amount of CR, just use the most simple biomarkers and forget about any animal studies in lifespan.
Crissman: Mm-hmm.
Michael: If you’re at some level of calories and you cut that by say 10%, 2,800 calories, you cut that to by 280 calories a day, now you’re 25, 20 a day. Are your biomarkers improved? What’s your glucose? Just using the very simple example, right? Glucose, right?
It increases during aging, with relatively higher levels associated with an increased all-cause mortality risk. If your glucose levels go from 107 on average fasting to 85 on a 10 % CR, and maybe that happens, maybe that doesn’t.
And your HbE1c drops from, I don’t know, 6.2 to 5.1, seems like calorie restriction in that case has put you on the path of metabolic health. Now, I’m not saying that will happen, but this is one way how we get closer to will any magnitude of CR be good for health and potentially longevity in people.
And if that is true, then it raises the question of what magnitude of CR may be best. And not just for glucose because it’s very easy to be reductionist and only focus on metabolic health, whether it’s glucose or lipoproteins, how do your kidney function markers look and your liver function markers?
And then the bigger question is, if you’re tracking your biomarker data over a few years, how does that compare to where it was before you were on CR? Have you slowed any rate of eight? So if you have three years of data without CR, then you have three years of data with CR, with say, you know, as I’m tracking eight blood tests per year, you can look at differences, you know, in, blood pressure and kidney function, liver function, HSCRP, does that data look better than where it did before?
And if it looks better, that would suggest that CR is a part of that approach, whatever magnitude of CR one might be on, is beneficial for health. Now, how does that translate? I don’t know, but I’d rather place my bet on the objective biomarkers of health rather than the absolutism of, you know, this has been shown to work, you know.
Michael: Many people right now are supplementing based on using a similar approach like AKG extends lifespan. But if you do that 900-day rule, the controls are short-lived and the supplemented group only extended lifespan in the female mice, not male mice.
But yet the majority of the longevity space is male-dominated, not female, you know, more males than females. Most of the people taking AKG are men, but yet the lifespan study that that’s based on it didn’t extend the lifespan in the male mice and the female mice.
They didn’t get past 900 days. anyway, it’s the same idea of not using an absolutism. It’s about looking, you know, use whatever intervention it may be, whether it’s CR or supplements or, you know, exercise prescription. What are the objective metrics? Collect a lot of data and then track that over time and see is your approach really beneficial, neutral, or detrimental. Just one last note.
So there’s a famous person in this space who posted his data, a lot of it today, with no dates on it, just, I’m the most quantified person in the world. These are my data. This is all the healthy stuff. Blood glucose was 74 and Hb1c was 4.5. Now, if you use the idea of, you know, like any net, well, you say impressive, but I’d argue the opposite side, because if you use the absolutist approach of
Crissman: Wow, impressive.
Michael: Calorie restriction, well that means that a BMI of 16, anorexia is gonna be longevity. No, that’s not what I’m saying. There’s nuance to this, right? So what does the published data show? So 80 to 94 lowest risk all-cause mortality. 74 is below that. For HbA1c, the all-cause mortality data is in giant meta-analyses, as many studies as you can collect.
Five to 6%. Now then, you could say, closer to five may be optimal relative to six. HbA1c increases during aging, but, in very advanced ages, the liver output of blood sugar, gluconeogenesis, liver function declines.
That’s one reason why LDL declines towards the end of life. So it’s possible that gluconeogenesis could be impaired, whether it’s extreme exercise or whether it’s an extreme magnitude of calorie restriction. And if that’s the case, the body’s ability to regulate blood sugar levels will be less good than it should be. So is 74 with an HbA1c of 4.5?
Better somehow, even though the published data suggests that that’s not the case. This is where the nuance comes into it, right? granted, his liver markers are youthful. I looked at those, so it’s not probably a liver story, and he’s probably not at increased all-cause mortality risk with the 74 and 4.5, but anyway, evaluating within that context is important. Biomarkers.
Crissman: Right. Well, right, you’re trying to get into round two already, Mike. We haven’t even finished round one here. So let’s just move on then until the next shot here. Because I think you’re over-relying on biomarkers.
Michael: Hmm.
Crissman: Okay. So biomarker tuning versus habit changes, which is the bigger gain?
Let’s talk about it.

So this is the slide that you wanted to bring up, but I think you just like slipped into this round before we even had the bell ring here. So I want to go ahead and present my case of it first and you can have your bottle. Is that fair? Okay. So this is the one of the biomarkers that you use, right? Again, I’m referring to your materials. This is the LaVine test.

Pheno age, which goes over a bunch of the biomarkers. And you were talking about some of these specifically. We have, let’s see, you’ve got the ALP in there, which is a liver enzyme. We’ve got the albumin, and also the glucose, which you just mentioned.
So in Levine’s test, basically the lower glucose is considered to be better and therefore longer, younger, more youthful. But if we take a look at glucose and the association between fast and glucose and all-cause mortality, some interesting things show up.

And this is where I think the biomarkers can lead you astray.

Like if you look at the change in fasting glucose as you get older, it goes up basically from around 84 up until about 96, depending on as your age goes by. And so we can take a look then and your glucose was something like 88 or something. So according to this table then that would give you an age of around 30 or something.
And you can say, I’m winning, I’m youthful, my glucose is lower than it is. But the same study goes on then to take a look and let’s see how all-cause mortality is related to glucose.

And so here we can see that basically the hazard ratio for the various different glucose levels are all virtually the same. Like around the area between, let’s say 80 to 105,
Crissman: It doesn’t matter what your glucose is, your premature death rate is virtually the same. It’s unaffected.
Michael: So wait real quick, 80 to 94 was the lowest risk. As you go above 94, risk significantly increases. So 94 is different from 105, and as you go below 80, that was associated with significantly increased risk.
So the lowest risk was 80 to 94, and then as you go above that on both sides of the U, significantly increased risk. So 105 is significantly higher than 94 with an increased risk.
Crissman: So are you referring to this study or a different study?
Michael: Yeah, this study. Very familiar with it.
Crissman: So you’re eyeballing that and you’re saying, wow, that’s a big risk there at 80.
Michael: No, I’m very familiar with this study. I’ve looked at the stats. 80 to 94 was the lowest all-cause mortality risk. As you go above 94, that is a significantly increased risk. And then even if you go back and others go back and take a look at that data and see that that’s exactly what it is, in terms of the hazard ratio when the triangle is completely above one, then it’s a significant association.
So if you look at that, it’s…just by eyeballing it, you can see that right before around 100, that’s the case where that triangle is completely above the hazard ratio of one. And then on the other side too, that starts to be true around 80, right? So just eyeballing it, you can see that that’s true. So anyway, sorry.
Crissman: Right, but you’re using the term significant in the technical sense of the word, which is to say statistically significant that you could retest and probably would have the same result. In common parlance, when you talk about the significance, you mean that you would actually notice as you would actually live a longer amount of time.
But the amount of the hazard ratio for that kind of number here, okay, if you squint at that, I have to look over towards where my sheen is, here, you could see that it is above the 1.0 line. But if you went through an intervention or you tried to change that, you would be changing your life in the manner of, what, minutes? Hours of expected lifespan?
Michael: Wait. So there’s another layer there. So glucose increases during aging. if your data, and remember this isn’t about one blood test. So if you’re looking at years of blood test data and you know, your data is where mine is on average around 90, then it’s 92, 94, 96, 98. You may look at that as, well, your risk, you know, you’re at 98, your risk is fine.
You’re within that, you’re within the quote-unquote reference range, which is less than, I don’t know, whatever it is in 105, you go to the doctor’s office, right? But your data is going in the wrong way. And that rate of change is potentially bad for health and life span.
If we’re talking about maximizing health and lifespan, I’d imagine being able to keep your glucose levels flat indefinitely will lead to the longest health and lifespan gain. Whereas if your data is 80 or 82, just go up two units every 10 years or 20 years, and your health has gotten worse, even though you’re still quote-unquote within range.
Now the other side of it too, as I mentioned, when considering that liver function declines towards the end of life, sure, maybe your data, you start to see it go from 90 to 88 to 84, but going in the other direction, right? And you think, higher is worse, right?
Yeah, but too low is bad too. And if that rate of change starts to put you at 76, 74, 68, you’ve probably got some liver, at least some liver-related issues going on.
However, the rate of change which is almost never reported in studies because it needs to be a longitudinal study with a lot of data for each person. Very rare. Sorry.
Crissman: Well, let’s take a look at that. you say that, okay, well, if it’s, let’s say that you are at say 90 and you think, okay, but that’s 90 now and maybe you’re 40 years old. But we saw that rate of change in the previous one here.
So if you’re 40 years old, let’s say you’re at 90, just natural aging, you could expect that your increase then, I mean, the entire range of this goes basically 12 points from 16 until over 60. And it doesn’t continue to increase much after the age of for men after the age of 52.
So if you have a 90 glucose at the age of 40, okay, maybe you’re gonna have a 93 at the age of 60 and then it stays there for the superior. And again, when you talk about the significance of this, mean, statistically significant, sure, but as far as a Hodges effect size or a D effect size, it’s gonna be a…
Michael: Wait, so the.
Crissman: virtually unmeasurable and unnoticeable. You’d be talking about less than months, maybe like a week or something of expected life change. I just don’t think it’s worthwhile to concern yourself with it.
Michael: Alright, so if you put it in perspective, let’s say your average glucose in your 20s is 84. Your average glucose in your 30s is 88. Your average glucose in your 40s is 92, right? Clearly the rate of change is going in the wrong direction.
Clearly your metabolic quote-unquote health in your 40s is worse than it was in the 20s. Now, you could make the argument, what does that translate into in terms of all-cause mortality risk? You could make the argument for health span, right?
Having your rate of age, the rate of change, go in the wrong direction, so where your 40-year-old metabolic health is not what it was in its 20s, but yet still, quote-unquote, healthy. For me, the goal is to be as youthful as possible, metabolically in all of the organs, as possible for as long as possible.
So I don’t wanna have a 92 average and be, quote-unquote, 10 years better relative to my chronological age. I want it to be at my best. So what will that translate into in terms of lifespan?
Who knows? if you fast forward and say, okay, now I’ve done this for 60 years and my average glucose is 90 for 60 years versus my rate of change has gone to the point where now my average glucose is 105. I mean, I’m gonna take the bet where having better metabolic health, just using this as an example, but kidneys too, liver, all of that, trying to keep the data as youthful as possible.
As naturally as possible, not artificially induced, will give me my best bet of not just health span, but also potential lifespan. It’s very difficult to quantify, you know because there aren’t any real studies. We’re looking at extrapolation based on curves.
But for me, it’s more of the philosophy of, you know that rate of change is bad because the rate of change, whether too high or too low, is truly aging. You’re aging. Now could say even though that’s within some quote-unquote healthy range, it’s still aging.
Michael: Now, if you’ve been able to keep it from aging and resist that age-related increase or decrease, that’s a win, right? Or if you’ve reversed it where, for example, my RDW was somewhere around 13 and I’ve flipped it down to 12, which is pretty close to optimal now, can I maintain that for the next 70 years, right?
So how much of a lifespan, and two, it’s also, it’s not just about one biomarker because maybe you’re right, maybe it’s just a one or 2 %…relative change in terms of all-cause mortality risk, but now multiply that by 20 biomarkers or 10 biomarkers, representative of all organ systems. Is that another 10 years of life? 30 years of life? 30? Nobody knows, right? So that’s the conquer aging or die trying bet.
Crissman: Well, that’s the then we can get back to the argument that you made before like what if someone is already an elite athlete Let’s say that they’re an elite athlete who also walks 12,000 steps a day Okay, so is then watching their glucose to try and get it from 96 down to 92 gonna be a worthwhile effort for them and give them a material gain. I don’t think so
Michael: So that’s up to the individual. mean, we all know the bed that I’m lying on. It’s not just about glucose. And also, when you consider that, we all know that elite athletes live longer than the average population, but it’s only five to seven years. my goal is to break the human longevity record, 122. So what’s the dose? What’s the dose of exercise? What’s the dose of all of it?
Crissman: Yeah
Michael: It’s got to be more than just eating real food and exercising because even the most well-intentioned people in this space, Jacqueline, died at 95 and he was talking about immortality forever and he was fit and functional forever. There’s got to be a higher level to this. You can even take it a step further.
What I’m doing is very basic of it. I’m looking at these markers of organ and systemic health, but then you can even titrate it down under the hood. If you take body composition and physical and cognitive function as the top tier.
Crissman: Yeah.
Michael: Now we’re back into tears and you subdivide that. There’s a whole bunch of stuff under that hood, right? So sure, I’ve proposed to take it a step further, you know, looking at cells and the proteins and even metabolites, creatinine is one example, but then you can go even further than that.
You know, it’s not just, you know, glucose and creatinine are metabolites. You know, our blood has like 4,000 metabolites that circulate. So even though I’m doing the metabolomics, you know, and that’s about 600 metabolites, you know, ideally, and I’m still subdividing that only into a handful of metabolites that I’m currently tracking.
Eventually, we’ll get to the point where we’re looking at entropy change from a healthy state, you know, so now it isn’t just a panel of 25 to 30 or 40 biomarkers, however much I’m using now to quote-unquote define youth and health.
We’ll have, you know, thousands of markers that are representative of the youthful state, and then we’ll have your current data to show how far is your have your, you know, have your quote unquote healthy state deviated from that? And then what can you do to get your full metabolism back to your healthy state or as much as possible?
So someone with someone that’s chronologically 60, maybe they can get back to the physiology and biochemistry of a 30-year-old. That’s the best they can do, right? So for me, it’s a data-driven process to try to enhance youth and everything else.
So, but if people don’t want to choose that and just want to go eat real food and exercise, you know, I’m not here to
be a fascist and say it has to be my way. Those who want to follow will follow and those who don’t, I mean, that’s their choice too.
Crissman: Yeah, need to get back to my argument before we need more mics out there doing the data to give us so we can go from a specific example to get a better view for it because I don’t I don’t think we’re gonna well, I mean, I think we will get there. As far as real longevity extension beyond 100 years old. That’s the Holy Grail at this point and
Honestly, my walking and exercise are not going to get me there. I’m not sure what the biomarkers are on there. I hope that you get to laugh at me sometime when you find out the biomarkers actually have completely conquered dying and aging and you live forever.
But I mean, the thing is, and this segues well into the next point, it comes to the new biomarkers, right? Like nowadays they talk about the methylation biomarkers, right?

So it’s kind of a more advanced thing where they’re talking about the activation of the genes.
But the most recent evaluation of it, and this is a white page, is still pre-peer review, it’s not been published. And this is made by the people who, basically the researchers came with a Dunedin pace methylation marker, which you do.

I think you had about 0.8 pace of aging. Mine was also comparable. We have a lot of similar habits. But the thing that is,
I’m not expecting people to read through all of this, but what I found to be fascinating about this is they look to see, what can we show. What interventions are shown to improve your epigenetics and show that you’ve reduced the speed of aging? And startlingly, you can see the vast majority of them don’t have any effect at all.
And right in the middle of this, they say that both diet and exercise have no effect on your DNA markers, right?
Forget walking 12,000 steps. They just say flat-out diet and exercise interventions had no impact on Dunedin Pace.
Michael: Can you share the full screen there because I don’t think on my end I can’t it’s very small We want to show that to the people
Crissman: It is quite small.
Michael: I can’t see it on my end. see the unaging. There we go. Yeah, yeah, yeah.
Crissman: Right, so it’s a right smack dab in the middle of it is one line, both exercise and diet, not shown to have any significant effect either way.
Michael: So I saw this preprint. I’m not surprised. In my data, calories currently aren’t significantly correlated with doneatum pace. So when you think about when you go all the way down in terms of the levels, right? So from that top-down, again, body composition and physical cognitive function, you could even say bone.
Bone is a part of body composition. If you go all the way down, you’ve got genomics. Can’t change our genetics currently. You go above that. Now we’re at epigenetics, which is one aspect of epigenetic modifications is methylation, which is what they’re measuring. You can also acetylate genes to turn them on or off.
So methylation is just one snapshot of that, right? So for those who don’t know, Dunedin PACE is not the best for asking the question, how old are you? What is your epigenetic age? There are other tests like the Horvat test, which is the gold standard for that. But it is significantly associated, with an older Dunedin PACE, a faster speed of epigenetic aging.
With an increased all-cause mortality risk and in the same ballpark as other gold standard clocks like phenology, the epigenetic phenology test, not the blood biomarker-based test.
In short story, long story short is that when you take the clinical biomarkers for Levine’s phenology and then you develop an epigenetic prediction of who’s younger, who’s older, and who’s in the middle, that’s the DNA methylation version of that. And then grim age, which is another gold standard clock, is consistently associated with an increased all-cause mortality risk.
So, Dunedin PACE is in the same ballpark for the effect size in terms of all-cause mortality risk, which highlights it as you know, clock for measuring the speed of aging. And then, one reason why it’s, you know, I’ve talked about it being potentially important, these other gold standard clocks like Horvath, FinoAge, and GrimAge, when you look at people on a calorie-restricted diet, only Dunedin PACE, for people on CR, it was 12 % CR, they weren’t overweight to start,
They were at the borderline of a BMI of around 25 and a year of randomized controlled trials. Dunedin-Pace was the only epigenetic clock able to identify a slower speed of aging relative to the other gold standard clocks. So that highlights that it’s potentially important.
Now, in terms of this study, the subject cohort means a lot. Are you looking at people who, for example, you know, ART therapy or kidney dialysis, you know, you do interventions, whether it’s diet, exercise, and this paper also looked at things like rapamycin, which I think wasn’t associated with a slowing of epigenetic aging either?
I think the subject, getting the subject population is important. For example, are you 80 years old and you’re taking rapamycin? What’s your epigenetic age? I don’t know, I haven’t looked. I don’t know if that’s included in this group of 51 studies. I’d expect that maybe that we’re.
would be where rapamycin as an example would have the greatest effect on people who have, you know, pre-existing conditions, rapamycin could be helpful. Now, if you have an elite athlete and they’re taking rapamycin, would you see a reduction in epigenetic aging? I don’t think that’s in this study either, right?
So the subject population is important and I think a lot of these cohorts aren’t exactly the fittest or healthiest. Now, this aside, it also goes back to how we can do this experiment on our own, right? We can try to find if calories or some magnitude of exercise is associated with a slower Dunedin pace.
And for me, like I said, calories aren’t associated right now and that’s after 17 tests. Yeah, yeah, now, but then it gets to the question of knowing that the DNA methylation-based test for phenology is a prediction of phenology, which includes the standard clinical chemistry biomarkers, albumin,
Crissman: Personally, okay. From your own tests, huh?
Michael: ALP, etc. For me, it makes sense. I want the actual data. don’t want the epigenetic prediction of that. But that said, I’m still a big fan of epigenetics. Don’t get me wrong. I love Hannah and Ryan, the heads of True Diagnostic.
They’re great. They’re fantastic. I love them in the field. They’re great. I’m not trying to knock them at all. But what biomarkers then is Dunedin Paste based on? Because it’s an epigenetic prediction of those biomarkers. So it includes 19.
Those biomarkers include things like VO2 max, waist-to-hip ratio, and gum health, so oral health is a part of that, APL-B, APL-A1, HbA1c, HSCRP, are all things that we can optimize towards youth and health without having the epigenetics.
Now, then it gets to, which aspects of diet can optimize the things that can be optimized on that list and which things can’t. So that’s where I’m currently at with that.
And looking at weak spots to try to make further gains in the need of pace. For example, my lipoprotein A has always been towards the higher end of the reference range. So I’ve been recently doing some experiments to try to bring my lipoprotein A down, which is thought to be genetically resistant to intervention, but in my data, that’s also not true.
I’ve been able to cut it in half at most. So anyway, that’s where I’m currently on that. But even there, you know, there may be some epigenetic pace of aging using Dunedin Pace where you get to a low level and you’re not able to go consistently below that.
For example, maybe 0.8 is the best that I can do based on my genetics, whereas others may be able to get up to 0.6 and they’re genetically able to have a slower pace of aging. So anyway, long story short is that we can, even without testing Dunedin Pace on your own, that list of 19 biomarkers, we can measure those things.
Even just leanness a high VO2 max, and good metabolic health, which are heavily dominant on that 19 biomarker list, optimizing that can go a long way towards potentially improving someone’s health and even slowing the pace of aging.
Crissman: So on that note, let’s go back to what you started with here. I haven’t looked at this too much. I recognize the rat chart, I think, that we just saw recently. But tell me about this. Is this your data? I wanted to know where it came from.
Michael: Yeah. All right. Yeah. So let me share screen here. Cause I gotta maybe, make it. Yeah. Yeah.
Crissman: is it better for me to let you share that?
Michael: Okay, bum bum bum. I don’t know if this is easier to see, but…
Bigger. All right, so this gets to the question of what magnitude of CR is CR potentially beneficial? And again, note for those who don’t know, my BMI is currently 22. Current calorie intake is around 2130. My ad-lib intake since 2015, I’ve weighed all my food. My highest intake which corresponds to any blood test, is 2800.
So when you take my current average intake and divide it by my ad-lib intake, that’s around 22, 23 % CR. I’ve tried to go lower than that. Some of my biomarkers get worse as we’ll see in a minute, but this idea of is CR better for biomarkers, right? So each of these circles is, corresponds to calorie intake. So, each biomarker that corresponds to a calorie intake. So for example,
If there’s a 50-day period in between blood tests because I’m tracking diet, I take the average 50 days for calorie intake and then that lines up with the latter blood test. I can do that for every blood test.
Now it has an average calorie intake and I can look at correlations. So for example, DHEA sulfate is an androgen. Androgens decline during aging. This is well known, DHEA included. So lower DHEA sulfate is going in the wrong direction. It declines during aging and is going in the wrong direction.
Michael: So here first, DHEA sulfate plotted versus DHEA sulfate y-axis plotted against calorie intake. In my data, we can see a significant correlation where higher calories are significantly correlated with lower DHEA sulfate.
So I’ve labeled that red. It’s going in the wrong direction. This would argue that higher calories is potentially bad for mechanisms that impact my production of DHEA sulfate. HSCRP, I don’t have to go through that. It’s higher, bad.
Higher calorie intake is significantly positively correlated with higher HSCRP. Higher neutrophils and monocytes, which increase during aging, and higher levels are associated with an increased all-cause mortality risk.
Higher calories there too, going in the wrong direction. LDL. So you can make the argument here a couple of ways. LDL follows an inverse U during aging, low in youth, peak at midlife, and low towards the end of life.
So, if your data is low, is it youthful or aged? In my data, LDL being higher tracks with more biomarkers going in the wrong direction than right. So higher LDL may be more reflective of the middle-aged data relative to the youthful data in my case.
And that’s a story I can go further in-depth on in terms of how you know if your data is middle-aged versus aged, but that’s a story for another day. Here, higher calories significantly correlated with higher LDL going in the wrong direction. Platelets.
Greater than 300 is U-shaped for platelets. So too low, less than 200, too high, greater than 300, increased all-cause mortality risk. So in my data, higher calories are associated with, significantly associated, these are P values less than 0.05 in a panel of about 25 standard clinical chemistry biomarkers.
So higher platelets. Now you could make the argument that platelets decline during aging. So this is resisting an age-related decline, but when considering that higher than 300 is going in the wrong direction and less than 200 is going in the wrong direction should have a closer to 200 or closer to 300.
The platelet story is similar to LDL for me where lower may be better, but even still we can leave this aside for now. RDW, I already showed that, but higher is worse, right? Higher calorie intake is significantly correlated with higher RDW.
Similarly for uric acid, uric acid increases during aging. Higher levels increase all-cause mortality risk. And that same story for systolic blood pressure. So we’ve got two, four, six, eight. What do we got? And then we’ve got two more that were at the top of the list here. Alkaline phosphatase values higher than 48 are associated with an increase in all-cause mortality risk. It may not increase during aging. There isn’t solid data for that.
And you can see that above 50, or 48, you can see higher calories and the correlation is significant. So that too going in the wrong direction and also HDL, higher calories significantly correlated with lower HDL. So I’ve got 10 biomarkers representative of many organ systems that are going in the wrong direction at a higher calorie intake.
And it isn’t just at the highest calorie intakes. You can see I have a spread of data that goes from around 2100 to 2800. Now there’s one exception to this and I only looked at significant correlations. Anything with a p-value greater than 0.05, I didn’t look at.
So higher calories are significantly correlated with higher lymphocytes. And that’s important because as I showed earlier, lymphocytes decline during aging, and values less than 2,000 as they go below that are significantly associated with an increased all-cause mortality risk.
So this suggests that there’s a calorie amount that may be optimal for lymphocytes but may be bad for 10 other biomarkers. So it gets to the question of and we’re considering that lymphocytes, at least in the mouse study, was one of the biomarkers that were associated with longevity, regardless of whether the mice were ad-lib, fasted, or on CR.
It then goes to the question of what magnitude of calorie intake and CR may optimize lymphocytes while not messing up the other biomarkers. And for me, that’s not my lowest calorie intake in 2080. I’m just a bit above that, right now 2130. In support of that, I’ve had two tests in a row where lymphocytes were closer to 1900, whereas, for the tests that were at my lowest calorie intakes, they were below 1600 for the first time in nine years.
But it gets to that idea of how to titrate the dose of calorie restriction. And using the biomarkers, at least in my case, I’ve got a multitude of biomarkers that are quote-unquote more youthful and healthy looking relative to higher calorie intakes.
Crissman: First of all, I gotta, I gotta applaud the data. mean, I can’t, I love it. that’s some, I like to have all those things, and going down to the P factor for each of them is very impressive. But, yeah. So you come, you come with, you come, you came with gloves and I come with gloves and kicks and jujitsu. And I got, I got all the skills in the toolbox.
Crissman: But I ain’t done yet. Because if you look those numbers though, the overall range that you’ve got there, mean, yes, I can see when you look at it that there’s a tilt to the line and as you say, it’s clearly showing that, okay, if you lose weight or if you’re in a lower calorie restriction, then you’re going to be going towards a positive side of it. But…
Michael: Okay, great, cool.
Crissman: I think all of those lines are fine for you in all ways, Mike. They’re all gonna be within the range. Like you’re already within the accepted range for all of them, aren’t you? Are any of those actually borderline to danger?
Michael: Nah.
Michael: To this, no, but when considering that they all change during aging, it’s basically, you know, it then I think the next question is actually, will the lower calorie intakes actually slow the rate at which those things change during aging? Right. And if that’s the case, then I’m onto something. So for, and you could say to like, okay, would 5 % CR make it that all right? So fine. You’re within the quote-unquote reference range but use the epi studies.
There are optimal ranges that are associated with the lowest all-cause mortality risk. There are values that are more likely to be found in youth. And based on all of those plots, my current magnitude of CR, around 20-something percent, low 20s, puts me on a road closer to youth and the lowest all-cause mortality risk. Now, how much of a lifespan or health span gain will I get? I don’t know.
Have I actually slowed the rate and pace of aging? If we look at just Morgan Levine’s phenology, and I covered this in…one of my most recent videos, blood test number seven, where phenyl age, if all biomarkers stay the same, you’ll have an increase by 0.9 years per year of chronological age. So in other words, starting four years ago, my biological age using that metric, and again, well, I’ll go through that in a minute, but 35.6 in 2020, okay?
So same biomarkers, if the biomarkers don’t change four years later, I should expect it to be 3.6 years older based on just the metric. So should be 35.6 plus 3.6, 39.2. 2024 current data is 34.8. So you could say I’ve resisted the age-related change. I’ve slowed some rate of aging, at least based on those nine biomarkers.
Their rate of aging over the past four years is slower than expected based on chronological age. So will that translate into five, 10? Nobody knows. This is the bet I’m making.
Michael: You know, and I’m happy for people to criticize and say, there’s no published data. I don’t, I don’t believe what you’re doing. Fine. Don’t don’t make your bet. Maybe I look, you know, so maybe I’ve got, so my dad’s brother died at 51. He had a stroke at 47. My dad’s father died at 67 heart disease.
My mom’s father, 67 heart disease. My mom’s brother, 67, whole bunch of stuff, kidney failure, everything, the whole gamut. So, if I don’t try to do what, you know, the Matt Damon line and the Martian if I’m gonna get out of this, I’m gonna have to science the shit out of aging. If I don’t try to take every bit of it, maybe my genetics will be dead by 80, even with the best well-intentioned biomarker and everything analysis.
I’m not gonna be mad at that, right? Maybe I’d push my lifespan longer than I would have naturally. I squeeze the orange as much as possible. But then maybe, just like Bernie Sanders says, maybe, but just maybe, I can really push this thing out, right?
Maybe I can discover, and continuously discover the recipe to keep my physiology and biochemistry as youthful as possible for as long as possible. And then I’m name-dropping like crazy using the Kurzweil, living long enough to live forever when real rejuvenation tech will come. Will that be in the next 70 years? Will it be in the next 500? I don’t know.
Crissman: I’m playing the same game on that one. think that we need to have the GLP-1 of longevity. that comes in and gives us sort of breaks it because all the interventions we have now, as we’ve talked about, they’re usually based on people who are not healthy, and what they’re able to offer someone who’s already living a healthy life isn’t enough. So go ahead, GLP-1, go.
Michael: So GLP-1, which is a satiety-inducing hormone, and this isn’t the only way. So for the people who hear me say this, tomato, tomato, right? Satiety, satiety, right? Maybe, anyway, so for the people who, I’m not trying to say this is the only way. There are a few ways we can activate GLP-1 without things like Olympic.
And one way is a high-soluble fiber diet. Soluble fiber produces gut bacteria, certain gut bacteria produce short-chain fatty acids from fiber fermentation and those short-chain fatty acids activate GLP-1 production. So now, then you could say, well, does fiber lead to a longer lifespan?
No animal studies. then, you know, there are no animal studies that have used a high soluble fiber diet. And, you know, what about human data, right? Well, most people barely get 20 grams of fiber, let alone five grams of soluble fiber. We may need 20 or 30 grams of soluble fiber.
Michael: Is it supplemental soluble fiber? Do I need to get it from vegetables, legumes, or other stuff, right? So there’s a whole bunch of questions there. So this is one reason why, and fortunately, the biomarkers seem to support this more often than not, but there is an upper limit here where my very high fiber diet of about 85 grams per day, about 20 of that being soluble, is a part of the overall approach for these mostly youthful biomarkers with some weak spots. Now, will that also help push past the…Nobody knows, there’s no data, right? So.
Crissman: You don’t supplement fiber, your diet is… Right. Same here, by the way. I mean, get my breakfast of whole grains and then on top of that the legumes and then some fruits and vegetables. But I know several of the other people who do recommend straight supplementation of it.
Michael: The issue there is, for whatever reason, there are animal studies and at least one human study that I know of where very high dose supplemental soluble fiber, for example, inulin, can induce liver cell damage, liver damage leading to higher ALT or AST in the blood. In one human study, RCT, they were with 30 grams of inulin per day. That’s 30 grams of soluble fiber per day. I mean, that’s more than I get whole food. It’s a lot.
Crissman: That’s a lot.
Michael: But the effect wasn’t in all study participants. three of the 18 people getting high dose inulin, the elevations in liver enzymes. So they had to stop taking, right? So, but there too, it gets the biomarkers. You’d have to actually measure and see if that’s making a dent like that, right? So there is an upper limit, you know, but.
Crissman: Yeah, let me by the way, I want to be careful and say that we’ve talked about the biomarkers and the utility of them. I want to be absolutely clear that there’s a huge benefit if your glucose level is far out of the range or treatment forward or your blood pressure and these other things. Oftentimes you and I are sort of talking about tweaking at the fine zone, right?
And I’m not sure that’s useful, but if you have high glucose or insulin issues or diabetes, other things, extremely useful to get the biomarkers and absolutely should be acted upon. So I think that it’s when we start to overturn and think that we’re able to then add additional life out of trying to take it down a few numbers or so, even though it’s already within the normal range. I think that’s the questionable part. So I just wanted to make sure that.
Michael: Yeah. So add, of course, yeah. So to add something to that, right? So imagine your HbA1c is 5.7, 5.8. Now we start to get into the pre-diabetic range. Now let’s say you went to your doctor, and your doctor says you’re pre-diabetic, you know, we’re gonna give you some metformin or some drug, right? But as a part of that process is gonna be regular monitoring to see what that reduces your HbA1c to, right? So regular monitoring is a big part of this approach.
Crissman: Listen to your doctors.
Michael: Then it gets to the question of what should my HbA1c be. And then it also raises the question of just like in the gym, how can I expect to improve my strength or performance if I’m not actively trying to make it better?
So if I’m not measuring my HbA1c and trying to keep it as youthful as possible, will it go in the age-related change range, and then I’m gonna be stuck having to take metformin or some other drug that may lose efficacy for years and decades of taking it?
Whereas if you’ve been trying to discover your own personal motorcycle recipe, maybe that’s the best approach for keeping it relatively youthful and resisting age-related change. But the only way to know that is by regular and repeated testing over a very long period of time so we can minimize that risk of getting to an advanced age.
And now it’s like, well, what do I do now? Even at that stage, you’re still going to have to start on that many test measurements. All I’m promoting is that let’s measure now. Let’s measure now. Let’s discover recipes now.
And wait, along those lines too, eventually, we’re gonna get to the point where, whether it’s in our toilets or finger prick or urinary, however, it may be, we’re all gonna have it where, you know, we’ll have a personalized health and exercise and sleep prescription based on our genetics, based on diet, based on air quality, based on all the things for recommended, you know, inputs per day that could potentially optimize our health and lifespan.
We’ll have…day-to-day integration, maybe even meal-to-meal integration. Now the question is when, how long will that take, right?
Crissman: Right. Well, as you talk about, then you find out that you need to take the habits. Can I jump into the update on the unaging challenge? Okay.
Michael: Yes. Yes. So how, so how, did, how does your, did your fight go? How do you think that went? Was it what you expected?
Michael: That’s my data.
Crissman: Yes, I’m going to, I mean, it’s a slideshow. I’ll get through this. So, first of all, thanks. I mean, as I said, I think we agree on most things. And so it’s fun to sort of pick on the things where I don’t think we do agree.
Yeah, you brought in some late-breaking news there. I wasn’t able to quite roll with that. So, you know, I’ll have to take a look at that. We might have to have a rematch or something to talk about that.
Michael: Yeah.
Crissman: But I think fundamentally your answers are right in that we don’t really know. And what we do know is that neither of us has a magic pill that’s guaranteed at this point. So I appreciate your experimentation. sure, and I think it’s, in my opinion, it would be sort of fine-tuning on the margins.
I think that there are better things and a better way that you could get the habits are the bigger drivers. And I know that you’re a believer in those habits as well. You live an exemplary life as far as your weekly workouts, your diet, and everything else. So I wouldn’t take away any of that part. I would say that I think you could shift your focus. I don’t know. What are your thoughts on our…
Michael: Wait, so, I know, know, sorry, sorry. I always have something to say, right? My daughter’s like, do you always have something to say? So just as an example of that, if I only focused on the habits, would my biomarkers be what they are now? And the fact is that’s not the case. When I first started on this journey in 2015, my liver enzymes were in the high thirties.
Now based on all-cause mortality risk, there too, there’s a U-shaped association where too low, increased risk. Low 20s, AST, ALT, lowest risk, and once you go above 22 or so, increased risk. My data was in the high 30s.
Now, wasn’t an alcohol drinker, which would be the obvious, what was going on there, but it was, my diet composition isn’t what it is now, and it’s only what it is now because I’ve been titrating over time to try to figure out the recipe to bring those liver enzymes down into the low 20s where they now currently are.
Michael: For whatever reason, in my case, too much omega-6 may have been part of that story. And this isn’t from seed oils. This is from walnuts and probably other nuts that I was eating at the time.
I may have a specific range where if I go above a certain amount for certain nutrients, it may induce liver damage. It may have been a fructose story where I was eating about twice as much fruit as I do now. And you’ve seen the strawberries. I mean, was eating double that.
Crissman: kilo, one pound of strawberries a day. Yep.
Michael: Well, back then it was strawberries and blueberries and blackberries. So it was double the intake then. So that may have been a contributor because high fructose, fructose is metabolized by the liver.
So you could say, it’s a whole food-based diet. There are no published studies that show increased mortality risk with increased fruit intake, right? So if I did nothing, I would have seen this unchecked maybe for the past 10 years, maybe putting me at an increased risk for liver disease. So this is…
That would be the argument where, you know, don’t assume that your diet and following the habits is the best approach. The only way to know is by looking at the biomarkers and objective tracking. But then once you start tracking, it’s like, okay, where are my weak spots and what can actually improve it, right? So.
Crissman: Come on, come on Mike, I’m kicking off the gloves. Keep on swinging, man.
Michael: All right. All right. No more swinging. I’ll take, I’ll take, yeah.
Michael: Look, someone eventually, I’m looking all the time for someone eventually will beat my approach, Schwarzenegger eventually got, there was an upgraded version of The Terminator, right? In The Terminator movies, right?
So, there’s only so long that I can do this before someone or some groups of people come along and beat this approach. I’m trying to cover every base, I’m very competitive, I try to cover every base, but someone will find a weakness and be better.
Crissman: Yep. Yeah.
Michael: If I die trying, well, then hopefully the field can move forward. And, you know, for example, just another quick example. One reason I developed this whole approach was seeing Jack Elaine and being a humongous fan, obviously, but I was like, there’s gotta be a better way. Even when he was saying eat real food and exercise, I was like, there’s gotta be a higher level.
And when he died, especially, was like, there’s gotta be a higher level. So what is the higher level? Someone is gonna come along and look at my stuff and be like, rudimentary, basic. This is a higher level than what Lustgarden was doing. So, and I look forward, I wanna learn from people like that, so.
Crissman: Right. So, when I talked before about the tiers of longevity, I think, well, you have some questions about the walking. think we agreed that the strength training, the aerobic and the high-intensity interval are key. So one of the things that I found, as I was, writing my blog and talking to people and, hoping to make an impact on their health and longevity.
That I got kind of a lot of understanding of it and yes, that seems like a good idea, but I didn’t really feel like people were actually doing that many of the things. So I’ve started the unaging challenge as I’ve talked about before in your blog posts, on your podcast, and in other places.
And at the moment we have 20 people who are currently going through the strength training section of it and moving on to the third challenge. So the unaging challenge is four separate challenges over the period of a year. And each of them focuses on a different aspect of your health.
We start out with aerobic and high-intensity interval training, then go into strength training, and then go into mobility and walking. And then the fourth challenge then is the personal peak where you make it your own. So we’re having a really great time. One of the big things about it is the sun is a community. So it’s not just a, do this by yourself.
There’s shared information and shared chat and other things. You can sort of hear how it’s going for other people and doing it as a challenge and it’s measured because you need to have measurement, of course, right? So how much you’ve lifted, what’s your one rep max, your VO2 max impact and other things so that you can actually track it over the period of the challenge? So the 20 early adopters, this is their many paths to strength.

So this is basically the effective total amount that they were able to lift in their calculated one repetition maximum based on what they did and you can see that there’s a whole different way of paths here as people went over the 12-week challenge of it It becomes a little cleaner if you look at it in terms of the people who were trained and the people who are untrained I was lifting before I started this so I’m on the blue line.

In general, the people who had already come into the unaging challenge strength challenge having lifted before, still were able to gain about 10 % through the unaging challenge system. For the newbies, they got to enjoy the beginner gains and they were able to increase about 40 % or so over time. Let me see if I’m…even more than that around 60 percent.
Naturally, some of them are just getting familiar with how you do the lift. When you come in for the first time obviously you’re not going to be attempting to do your maximum lift when you’re just getting used to how you move the dumbbell around or or do the exercises.

So we almost have a hundred people registered for the 2025 challenge and if anyone is interested we still have open registration. It is completely free. I believe this kind of information should be available to everyone. While unfortunately, I can’t clone Mike Lustgarten to duplicate his data, we can get together and work together on the unaging challenge. So the data is tracked.
For example, the 20 people during the strength challenge, the total amount lifted is over 1.5 million tons, which is the weight of a jumbo jet.

So this is an artistic representation of the 20 early adopters and what we’re able to achieve during that time.
So if you’re interested in more information, you can transform yourself.
The challenge starts on January 6th and we’ll be putting you into a group with other people. It’s just a way of spreadsheets so that you can see sort of what they’ve done and they’ll be able to see what you can do and also encourage each other through the challenge. And you can find that at unaging.com.
And then under the challenge, can do registration for that and then we’ll take it from there. So I don’t know, any comments or questions on the unaging challenge?
Michael: Yeah, no, that was great. I was gonna, you know, give you a shout-out and promote unaging.com and the unaging challenge, but you did a great job of promoting it. So hopefully people, if they’re interested, will check it out and sign up and be a part of it. So.
Crissman: Trying to move the world. Okay, all right. Anything else we should cover before?
Michael: Yes.
Michael: Yeah, I guess we’ll talk about the aliens next time. Yeah. All right, cool. Ciao, Criss.
Crissman: So much to talk about. Okay. All right, great. Thank you very much for the chance to talk.









